Health Is Attainable at Any Age: A Personalized Approach to Men’s Hormone Health
Clinical Summary for Providers
- Testosterone deficiency assessment extends beyond total testosterone alone, incorporating symptom burden, free testosterone, SHBG (sex hormone-binding globulin), and broader patient context.1
- Pathway selection is individualized, with factors that include TRT (testosterone replacement therapy), enclomiphene, fertility priorities, and protocol-specific monitoring.1
- Men’s hormone health frequently extends beyond androgen support, with body composition, sexual wellness, metabolic factors, and adjunctive strategies often entering the discussion.2
- Monitoring is central to long-term management, including parameters such as hematocrit, PSA (prostate-specific antigen), tolerability, and individual response.1
- Individualized care utilizes personalized medicine frameworks to tailor medication and care plans to the specific needs and context of the patient.3
How Providers Can Help Patients Pursue Precision-Informed, Individualized Care
During Men’s Health Month, conversations around prevention, vitality, and long-term health bring renewed attention to men’s hormone health. Too often, they’re anchored to average baselines despite the need for more nuanced thinking. As providers increasingly challenge inherited assumptions in care, a larger question emerges: is the goal simply to fall within range, or to pursue more tailored support?
In many ways, defying the odds in men’s hormone health begins by moving beyond the status quo of average.
As testosterone optimization continues to evolve, providers are navigating questions around diagnosis, fertility priorities, pathway selection, and ongoing monitoring. Those questions rarely point to one standardized answer and instead require sound provider judgment.
Moving Beyond Average Baselines in Men’s Hormone Health
Men’s hormone health is often reduced to a single value or isolated symptom. In practice, providers assess symptoms, biochemical findings, metabolic context, and patient-specific goals as part of individualized clinical evaluation.
Contributing factors providers may evaluate can include:
- Sleep and stress burden
- Nutrient status
- Metabolic factors and comorbidities
- Potentially reversible contributors to symptomatic presentations
A broader clinical lens may help distinguish whether a presentation reflects testosterone-related concerns, systems-level contributors, or both.4
“Defying the odds in men’s hormone health begins with defying one-size-fits-all thinking.”
A Diagnostic Framework for Evaluating Testosterone Concerns
Evaluating testosterone concerns requires more than aligning to a single threshold. Provider consultations involve symptom assessment alongside biochemical confirmation and broader patient context.
Considerations typically include:
- Total testosterone and free testosterone interpretation5
- SHBG evaluation5
- LH (luteinizing hormone) and FSH (follicle-stimulating hormone) evaluation5
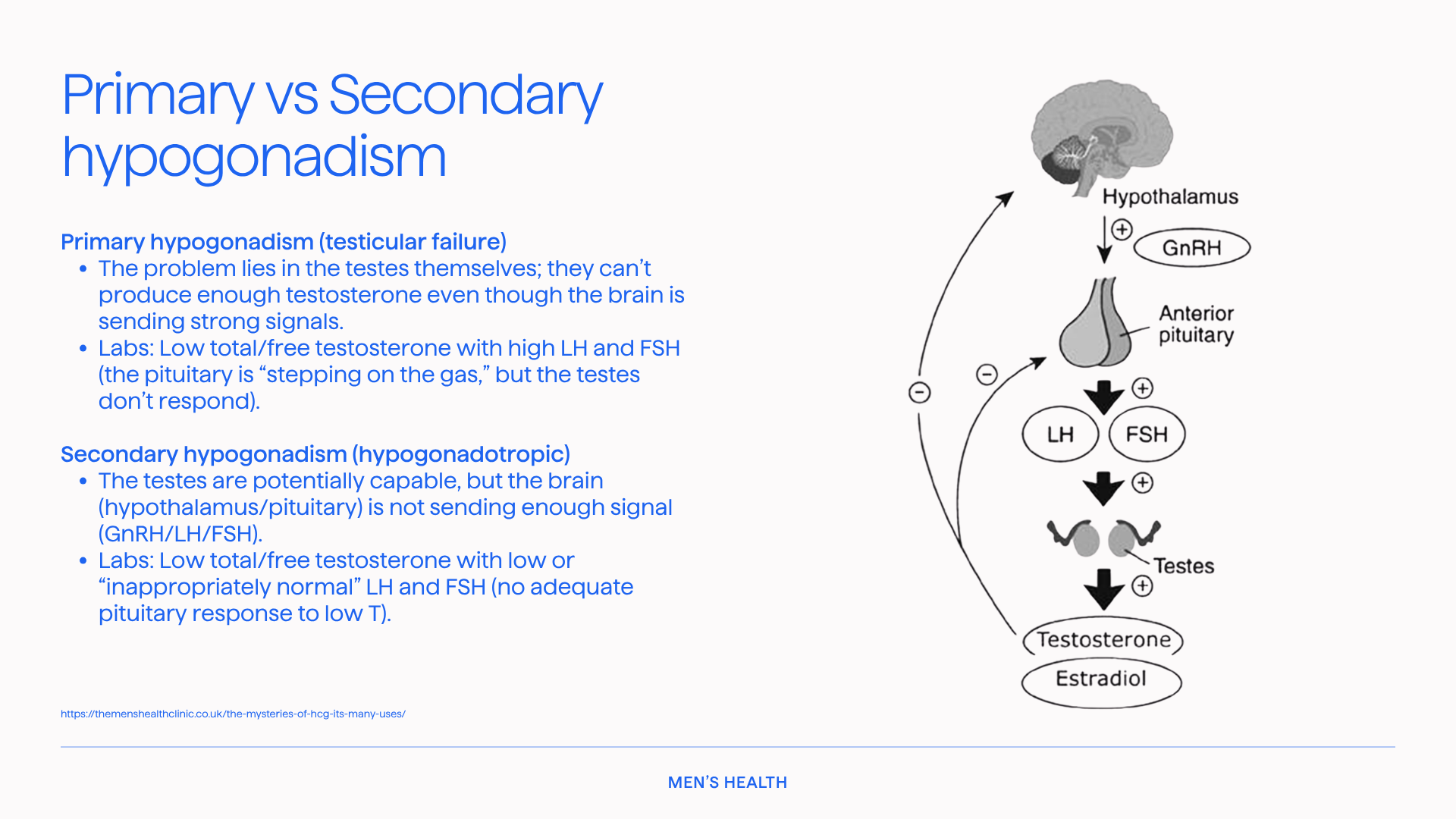
- Distinguishing primary vs secondary hypogonadism5
- Borderline presentations that may require deeper context5
Standardized thresholds inform care, but individualized interpretation defines it.
Clinical Care Plans for Testosterone Optimization
If diagnosis is where nuance begins, pathway selection is where it becomes practical.
Exogenous Testosterone Formulation Approaches
Compounded pathways may include injectable, transdermal, and oral or buccal formulations, each with distinct practical implications within individualized care planning. Emerging oral compounded formulations, such as Testosterone LPT® tablets, utilize liposomal delivery platforms designed to support drug stability and absorption while addressing challenges associated with oral testosterone delivery.6
Rather than viewing these as interchangeable options, providers consider them as tools within tailored care plans. The objective is not choosing from standardized protocols, but selecting the right option for the right patient context.
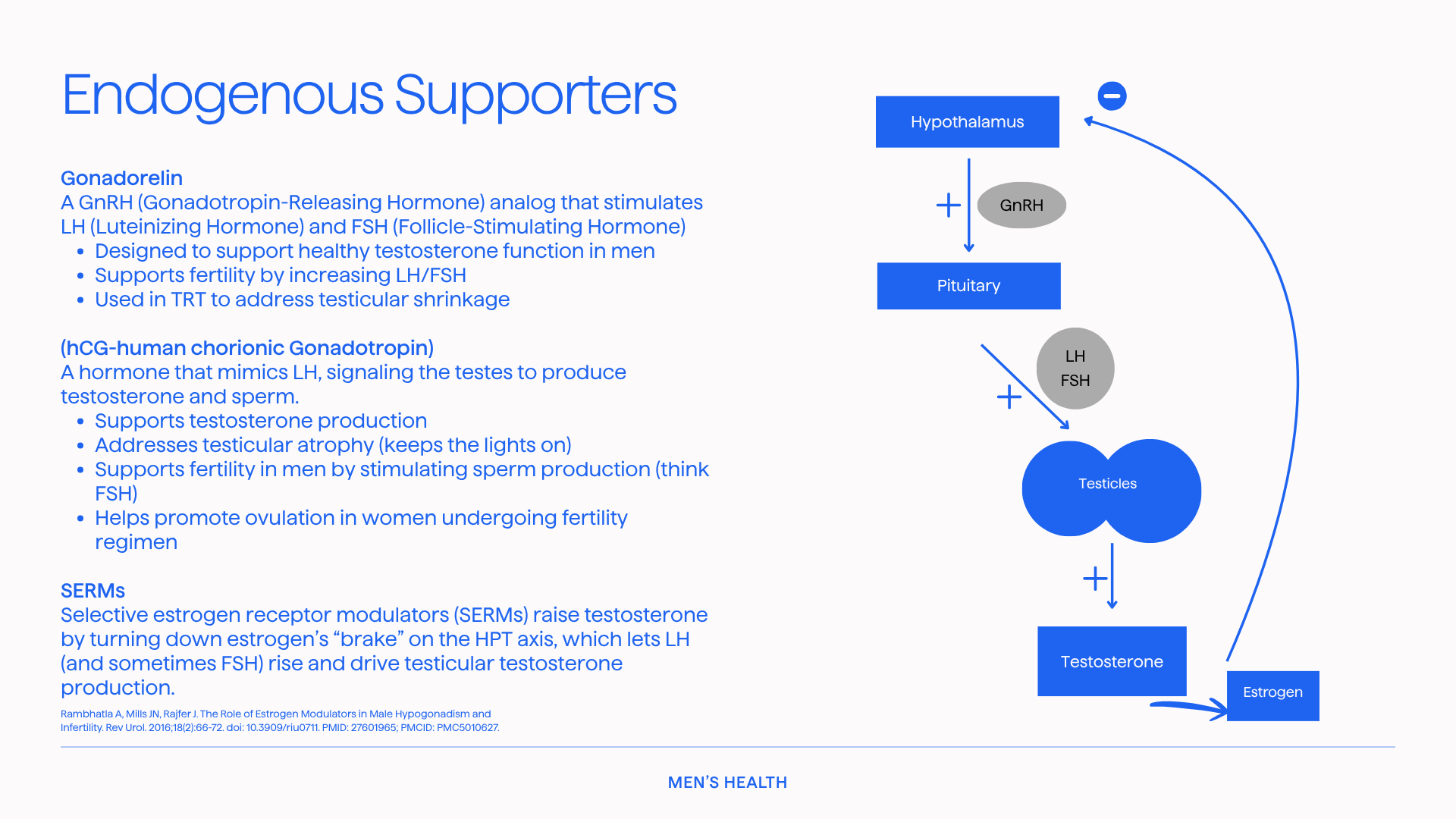
Supporting Endogenous Testosterone Function
In appropriate patients, strategies to support endogenous testosterone production may also be considered. Enclomiphene is often central to these discussions, particularly in patients where preserving endogenous production or fertility is a priority. These considerations may also include broader SERM-based strategies, as well as supportive options such as hCG or gonadorelin where relevant.8
This is where the conversation expands beyond either-or thinking and toward supporting formulation fit.
How Fertility Priorities Shape Provider Decision-Making
One-size-fits-all discussions can be especially limiting when fertility goals are part of the picture.7
For some patients, family-building priorities shape:
- Counseling discussions
- Pathway considerations
- Timing decisions
- Monitoring priorities
A heart-led approach to care often begins by understanding what matters most to the patient, then letting those goals inform decisions.
Technical rigor and patient context must work together.
Adjunctive Approaches Beyond Primary Options
Men’s hormone health conversations extend beyond primary options alone.
Foundational elements commonly include:
- Sleep as a testosterone-supportive variable9
- Resistance training and body composition factors5
- Management of comorbid factors where relevant9
Thoughtful care is strengthened not only by what is prescribed, but by what surrounds the care plan.
Muscle Health, Sarcopenia, and Recovery in Men’s Hormone Care
Men’s hormone health can intersect with body composition, functional strength, and age-related muscle changes, including sarcopenia. In practice, these conversations are often framed within a broader physiologic context rather than isolated to a single pathway, and may include compounded sermorelin formulations in broader muscle health and body composition discussions.10 These discussions reinforce that men’s health may benefit from a multidimensional approach rather than isolated categories.
Sexual Wellness as Part of Individualized Men’s Health Care
Sexual wellness concerns can also intersect with broader men’s health assessments.
In many cases, these concerns reflect underlying hormonal, vascular, metabolic, or psychological factors that warrant a broader physiologic lens.11
In appropriate patients, discussions may include compounded tadalafil and other compounded formulation approaches, often in the context of vascular function, endothelial signaling, and symptom-specific considerations. Compounded combination formulations, such as Olympus (for sexual wellness), may also enter these discussions, incorporating multiple pathways across vascular, central, and neuroendocrine signaling that may be relevant to sexual function.12
For providers, sexual wellness conversations often serve as an entry point into deeper discussions around hormone health, metabolic function, and overall vitality. Framed within patient-specific goals, they can guide more individualized decision-making.
Metabolic Context in Men’s Hormone Health
Broader metabolic evaluations may include compounded NAD+ formulations and their role in cellular energy processes.13
As men’s health continues to evolve, providers increasingly frame hormone discussions within a broader systems-level context, recognizing the potential interplay between metabolic function, mitochondrial activity, and overall physiologic balance.
In some patient contexts, these discussions extend to how energy metabolism, oxidative stress, and lifestyle factors may intersect with patient presentation.
Monitoring for Tolerability and Individual Response
Monitoring is a central component of pathway selection.
Baseline evaluation, follow-up laboratory review, and ongoing reassessment support provider decision-making over time.
Providers may assess:
- Hematocrit and PSA parameters
- Individual response
- Patient progress
- Tolerability
- Alignment between goals and care plan
In individualized care, follow-up is where care strategies are defined and refined.
Car Plan Summary for Providers
Key factors include:
- Diagnostic confirmation beyond total testosterone alone
- Distinguishing primary vs secondary hypogonadism
- Fertility priorities prior to pathway selection
- Care plan approaches for exogenous and endogenous-supportive strategies
- Monitoring for tolerability, patient progress, and individual response

Defying the Odds in Men’s Health Through Individualized Care
Men’s hormone health extends beyond selecting between interventions. It involves evaluating care through the lens of diagnosis, fertility priorities, supportive strategies, and monitoring for individual response.
Supporting health at any age begins with provider decision-making grounded in patient-specific goals.
Men's Health Month is a timely reminder: advancing men's health means challenging average baselines and rejecting standardized care plans in favor of informed, patient-specific care.
Personalized medicine isn't an add-on. It's the foundation.
For providers committed to this approach, the invitation is clear:
Defy the odds by defying the average.
Clinical FAQs
What is the standard diagnostic threshold for testosterone concerns?
While a total testosterone threshold below 300 ng/dL is often referenced, evaluation also includes free testosterone, SHBG, symptom burden, and broader patient context rather than relying solely on a binary biochemical cutoff.
How do providers approach TRT versus enclomiphene pathways?
Pathway selection depends on etiology, fertility priorities, symptom presentation, formulation preferences, and monitoring factors.
What monitoring parameters are considered in testosterone care plans?
Clinical evaluations typically include hematocrit, PSA, estradiol, metabolic markers, and individualized follow-up intervals.
Disclaimers:
The information provided in this blog article is for informational and educational purposes only. Refer to the cited references for more information regarding the content presented. The information in this blog article is not intended as a substitute for professional medical advice, diagnosis, or treatment. Never disregard professional medical advice or delay seeking medical attention because of something you have read in this blog article. The creators of this content disclaim any liability for decisions made based on the information presented.
Consult your healthcare provider before starting any over-the-counter (OTC) products or prescription medications. Always seek the advice of your healthcare provider for any questions you may have regarding a medical condition. Certain medications may interact with your current prescription medications, medical conditions, or other supplements. Your healthcare provider can provide guidance tailored to your specific health needs.
Compounded medications are not approved by the FDA and these statements have not been evaluated by the FDA.
References
- Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018;200(2):423-432. doi:10.1016/j.juro.2018.03.115
- Muraleedharan V, Jones TH. Testosterone and the metabolic syndrome. Ther Adv Endocrinol Metab. 2010;1(5):207-223. doi:10.1177/2042018810390258
- Delpierre C, Lefèvre T. Precision and personalized medicine: what their current definition says and silences about the model of health they promote. Implication for the development of personalized health. Front Sociol. 2023;8:1112159. doi:10.3389/fsoc.2023.1112159
- Khera M, Torres LO, Grober ED, et al. Male hypogonadism: recommendations from the Fifth International Consultation on Sexual Medicine (ICSM 2024). Sex Med Rev. 2025;13(4):548-573. doi:10.1093/sxmrev/qeaf036
- Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. doi:10.1210/jc.2018-00229.
- Liu P, Chen G, Zhang J. A Review of Liposomes as a Drug Delivery System: Current Status of Approved Products, Regulatory Environments, and Future Perspectives. Molecules. 2022 Feb 17;27(4):1372. doi: 10.3390/molecules27041372. PMID: 35209162; PMCID: PMC8879473.
- Brannigan RE, Hermanson L, Kaczmarek J, Kim SK, Kirkby E, Tanrikut C. Updates to male infertility: AUA/ASRM guideline. American Urological Association guideline. J Urol. Published online August 15, 2024. doi:10.1097/JU.0000000000004180.
- Ramasamy R, Armstrong JM, Lipshultz LI. Preserving fertility in the hypogonadal patient: an update. Asian J Androl. 2015;17(2):197-200. doi:10.4103/1008-682X.142772.
- Liu PY, Reddy RT. Sleep, testosterone and cortisol balance, and ageing men. Rev Endocr Metab Disord. 2022;23(6):1323-1339. doi:10.1007/s11154-022-09755-4
- Johannsson G, Svensson J, Bengtsson BA. Growth hormone and ageing. Growth Horm IGF Res. 2000;10(suppl B):S25-S30. doi:10.1016/S1096-6374(00)80006-4
- Simopoulos EF, Trinidad AC. Male erectile dysfunction: integrating psychopharmacology and psychotherapy. Gen Hosp Psychiatry. 2013;35(1):33-38. doi:10.1016/j.genhosppsych.2012.08.008
- Aversa A, Vitale C, Volterrani M, et al. Chronic administration of tadalafil improves endothelial function in men with increased cardiovascular risk. Eur Urol. 2007;47(2):214-220. doi:10.1016/j.eururo.2004.10.002
- Castro-Portuguez R, Sutphin GL. Kynurenine pathway, NAD+ synthesis, and mitochondrial function: targeting tryptophan metabolism to promote longevity and healthspan. Exp Gerontol. 2020;132:110841. doi:10.1016/j.exger.2020.110841.