By Rex Jones, PharmD, clinical pharmacist specializing in peptide therapeutics and provider education.
Understanding Peptide Pharmacology
Traditional pharmacology frameworks were largely built around small molecule drugs, and peptide pharmacology doesn't always follow the same playbook.
That doesn’t mean peptides operate outside the rules of pharmacology. It means some of the assumptions providers commonly rely on—especially around plasma concentration, biologic duration, delivery strategy, and dose interpretation—may not always translate neatly into peptide regimens.
Peptide pharmacology examines how peptide compounds interact with receptors, signaling pathways, pharmacokinetic systems, and downstream physiologic responses. Unlike many traditional small molecule drugs, peptides are often characterized by receptor-mediated signaling dynamics, delivery constraints, and downstream physiologic amplification.1
Their activity often involves receptor activation, intracellular signaling cascades, signaling persistence, and physiologic variability that extend beyond simple plasma exposure.
As provider interest in peptides continues expanding across metabolic support, endocrine physiology, tissue signaling research, and broader personalized medicine conversations, understanding peptide pharmacology becomes increasingly important.

Key Concepts in Peptide Pharmacology
- Peptide signaling may persist after measurable plasma exposure declines
- Peptide pharmacokinetics and pharmacodynamics may not align cleanly
- Delivery method may materially influence peptide signaling behavior
- Peptide medications often exhibit substantial physiologic variability among patients
- Traditional exposure-response assumptions may not fully explain peptide activity
What Makes Peptides Structurally Different?
Peptides are short chains of amino acids, the same molecular building blocks that make up proteins.
However, peptides are generally much smaller and less structurally complex than proteins. While proteins may contain hundreds or thousands of amino acids folded into highly intricate structures, peptides are typically shorter sequences that often function as biologic signaling molecules.
That signaling role matters pharmacologically.
Many endogenous peptides regulate physiologic communication throughout the body. Endogenous peptides such as insulin, glucagon, oxytocin, and vasopressin all function within broader signaling networks tied to metabolism, endocrine activity, fluid balance, reproduction, and cellular coordination.1
Even small changes in peptide sequence may alter receptor binding behavior, signaling intensity, receptor selectivity, and downstream biologic activity. In practical terms, peptide structure and physiologic function are tightly linked.2
This is one reason peptide science continues generating substantial clinical and research interest.
How Peptides Interact With Cellular Receptors
Many peptide drugs exert their activity through cell surface receptor-mediated signaling pathways rather than passive intracellular diffusion.1
Once receptor binding occurs, the receptor undergoes structural changes that initiate signaling cascades inside the cell. Those cascades may then amplify the original signal to produce functional changes and coordinate broader physiologic responses.
Receptor Signaling Pathways
Several receptor types commonly associated with peptide receptor signaling include:
- G protein-coupled receptors (GPCRs)
- Receptor tyrosine kinases
- Cytokine receptor signaling pathways
These systems may participate in:
- metabolic signaling
- endocrine communication
- immune modulation
- cellular maintenance
- tissue signaling processes
Importantly, these pathways do not operate in isolation. Receptor cross-talk, signaling overlap, receptor desensitization, and receptor internalization dynamics may all influence how peptide activity unfolds over time.3
Receptor desensitization is particularly important clinically because repeated signaling exposure may alter receptor responsiveness over time. This is one reason peptide response may not always remain static even when dosing remains unchanged.
That complexity is part of why simplified pharmacologic models often fall short when interpreting peptide mechanisms.
Why Peptide Signaling Behaves Differently
One of the most clinically important distinctions in peptide pharmacology is that plasma concentration and biologic signaling duration may not always align cleanly.
In traditional pharmacology discussions, plasma exposure is often used as a rough proxy for biologic activity. With peptide compounds, the relationship can become more layered.
Once receptor activation occurs, downstream signaling cascades may continue unfolding after the peptide itself is no longer present at meaningful circulating levels.
That downstream activity may involve:
- secondary messenger systems
- phosphorylation cascades
- transcription signaling
- cellular amplification pathways
- coordinated tissue-level signaling responses
Rather than functioning purely through constant receptor occupancy, peptide drugs may initiate signaling events that continue propagating downstream after the initial receptor interaction.
“The peptide no longer has to be present at the receptor on the cell surface for these cascades to be ongoing.”— Rex Jones, PharmD, Strive Pharmacy
This creates a potential pharmacokinetic and pharmacodynamic mismatch.
In other words:
Measurable peptide concentration and functional biologic signaling are not always the same thing.
A Practical Example: GLP-1 Receptor Agonists
GLP-1 receptor agonists provide one recognizable example of how peptide pharmacodynamics may extend beyond simple plasma concentration alone.
In literature, the activation of endogenous GLP-1 signaling pathways may influence insulin secretion, gastric emptying, appetite regulation, glucagon signaling, and central satiety pathways, each operating through layered downstream physiologic mechanisms. While plasma pharmacokinetics remain clinically important, downstream physiologic response may not always correlate perfectly with circulating drug concentration at a single time point.4,5
This does not make plasma exposure irrelevant. It illustrates how peptide signaling may involve broader physiologic coordination beyond simple concentration-response assumptions alone.
That distinction shapes how modern peptide pharmacology is discussed and applied.
Peptide Pharmacokinetics vs Pharmacodynamics
Traditional small molecule pharmacology often assumes a relatively straightforward relationship between plasma concentration and biologic activity. Peptide pharmacology may behave differently.
Peptide pharmacokinetics frequently involve:
- rapid enzymatic degradation1
- shorter plasma half-life1
- membrane permeability limitations1
- delivery-related bioavailability challenges1
At the same time, peptide pharmacodynamics may involve signaling cascades that continue evolving after measurable plasma exposure declines.
That gap between measurable exposure and downstream signaling activity is one reason clinical interpretation of peptide regimens often requires broader context than pharmacokinetic data alone can provide.
As a result, providers may not always have a straightforward laboratory marker capable of fully capturing how peptide-related signaling is unfolding physiologically.
This may partially explain why peptide protocols can produce substantial variability across both research settings and real-world clinical practice.
Clinical interpretation often requires a wider lens, including:
- functional response
- administration strategy
- dosing frequency
- physiologic variability
- patient-specific goals
- overall clinical context
Why Delivery Method Matters With Peptides
With peptide drugs, delivery strategy is not simply a convenience issue. It is often central to how exposure and signaling behavior are interpreted.
Because peptides frequently exhibit limited membrane permeability and enzymatic degradation susceptibility, administration route may significantly influence:
- absorption behavior1
- exposure stability1
- tissue access1
- dosing practicality1
- overall regimen design1
Subcutaneous Administration
Subcutaneous administration remains one of the most commonly discussed systemic delivery approaches because it may support more stable exposure patterns while remaining practical for repeated administration schedules.1
Intranasal Delivery
Intranasal delivery continues generating interest where central nervous system access is being explored.6
Oral Peptide Bioavailability Challenges
Oral peptide delivery remains an active area of formulation research because gastrointestinal degradation creates substantial bioavailability challenges for peptide compounds.7
This is one reason peptide formulation science continues advancing alongside peptide pharmacology itself. Delivery systems, absorption characteristics, and exposure patterns may materially influence how peptide signaling behaves physiologically.
Why Peptide Response Can Vary Between Patients
Peptide signaling does not occur inside a standardized physiologic environment.
Two patients receiving the same peptide regimen may not exhibit identical receptor sensitivity, signaling behavior, downstream pathway activation, or functional response patterns, even when dosing appears similar.8
Several factors may contribute to this variability, including:
- receptor expression differences
- signaling sensitivity variability
- physiologic state differences
- administration preferences
- dosing frequency tolerance
- broader metabolic and endocrine context
This creates another important distinction from simplified dose-response assumptions often associated with traditional pharmacology models.
Standardized pharmacokinetic frameworks alone may not fully explain how peptide signaling translates physiologically from patient to patient.
That does not make peptide pharmacology unscientific. It makes biologic interpretation more layered.
As a result, peptide dosing strategies often rely on a combination of:
- mechanistic reasoning
- evolving clinical interpretation
- formulation considerations
- patient-specific context
- broader physiologic assessment
Peptide research continues evolving rapidly, but standardized interpretation frameworks remain limited across many areas of clinical practice. Peptide regimens often rely heavily on mechanistic rationale, signaling theory, and real-world clinical observation rather than long-term outcomes data.
Peptides & the Future of Personalized Medicine
Peptide science continues expanding across multiple areas of modern medicine research and clinical interest, including:
- metabolic signaling
- endocrine physiology
- immune modulation
- reproductive physiology
- cardiometabolic systems
- tissue signaling research
At the same time, peptide development itself continues evolving.
Researchers are exploring:
- longer-acting formulations
- oral delivery technologies
- receptor selectivity refinement
- increasingly targeted signaling approaches
- more sophisticated delivery systems
As peptide science advances, providers may need to look beyond traditional pharmacologic models when evaluating how peptide signaling behaves clinically.
Watch our Peptides Webinar | Strive Sessions
Peptide Pharmacology FAQs
What is peptide pharmacology?
Peptide pharmacology examines how peptide drugs interact with absorption systems, receptors, signaling pathways, and downstream physiologic processes. Unlike many traditional small molecule drugs, peptides frequently operate through receptor-mediated signaling mechanisms that may produce more complex pharmacokinetic and pharmacodynamic behavior.
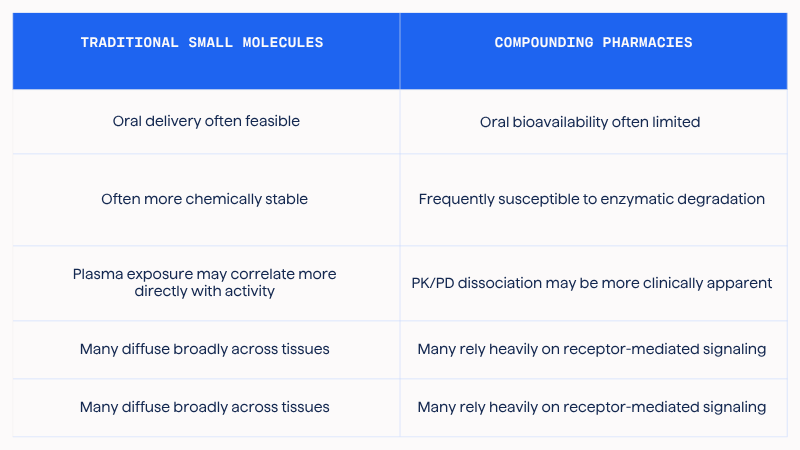
How do peptide drugs differ from traditional drugs?
Many traditional drugs are small molecules that diffuse broadly throughout tissues or interact through more direct exposure-response relationships. Peptide drugs often rely heavily on cell surface receptor-mediated signaling pathways that may produce layered downstream physiologic responses.
Why can peptide signaling persist after plasma levels decline?
Once receptor activation occurs, peptides may initiate downstream signaling cascades involving secondary messenger systems, phosphorylation pathways, transcription signaling, and broader cellular responses. In many cases, those downstream processes continue after measurable circulating peptide levels decrease.
Why is peptide half-life difficult to interpret?
Plasma half-life does not always fully capture biologic signaling duration with peptide drugs. Peptides may degrade rapidly in circulation while downstream signaling activity continues evolving after the original receptor interaction occurs.
Why does peptide delivery method matter?
Peptides are often susceptible to enzymatic degradation and may exhibit limited membrane permeability. As a result, the administration route may significantly influence absorption behavior, bioavailability, exposure stability, and signaling activity.
Why can peptide response vary between patients?
Peptide signaling may be influenced by receptor expression, signaling sensitivity, physiologic state, metabolic context, administration strategy, and dosing frequency. Two patients receiving the same peptide regimen may not exhibit identical physiologic responses.
What makes peptide pharmacokinetics different?
Peptide pharmacokinetics may involve rapid enzymatic degradation, shorter plasma half-life, and delivery-related bioavailability challenges. In some situations, pharmacodynamic signaling activity may persist beyond measurable plasma exposure.
Are peptide pharmacodynamics always predictable?
Not necessarily. Peptide pharmacodynamics may involve layered signaling cascades, receptor dynamics, physiologic variability, and evolving mechanistic interpretation frameworks that do not always behave according to simplified linear exposure-response assumptions.
What are the biggest challenges in peptide pharmacology?
Some of the biggest challenges in peptide pharmacology include interpreting pharmacokinetic and pharmacodynamic relationships, understanding signaling persistence after plasma decline, managing delivery-related bioavailability limitations, and accounting for substantial variability between patients.
How are peptide medications metabolized?
Many peptide medications are metabolized into amino acids through enzymatic degradation pathways involving proteolytic enzymes throughout circulation and tissues. This can contribute to shorter plasma half-life and delivery-related formulation challenges.1
Disclaimer:
The information provided in this blog article is for informational and educational purposes only. Refer to the cited references for more information regarding the content presented. The information in this blog article is not intended as a substitute for professional medical advice, diagnosis, or treatment. Never disregard professional medical advice or delay seeking medical attention because of something you have read in this blog article. The creators of this content disclaim any liability for decisions made based on the information presented.
Consult your healthcare provider before starting any over-the-counter (OTC) products or prescription medications. Always seek the advice of your healthcare provider for any questions you may have regarding a medical condition. Certain medications may interact with your current prescription medications, medical conditions, or other supplements. Your healthcare provider can provide guidance tailored to your specific health needs.
Compounded medications are specially prepared for individual patient needs based on a valid prescription and, as such, are not reviewed or approved by the U.S. Food and Drug Administration (FDA) for safety or efficacy. These statements have not been evaluated by the FDA.
References
- Wang L, Wang N, Zhang W, et al. Therapeutic peptides: current applications and future directions. Signal Transduct Target Ther. 2022;7(1):48. doi:10.1038/s41392-022-00904-4
- Kim J, Kim J, Choi C, et al. Structural insights into GPCR signaling activated by peptide ligands: from molecular mechanism to therapeutic application. Exp Mol Med. 2025;57:1467-1481. doi:10.1038/s12276-025-01497-y
- Flores-Espinoza E, Thomsen ARB. Beneath the surface: endosomal GPCR signaling. Trends Biochem Sci. 2024;49(6):520-531. doi:10.1016/j.tibs.2024.03.006
- Girada SB, Kuna RS, Bele S, Zhu Z, Chakravarthi NR, DiMarchi RD, Mitra P. Gαs regulates glucagon-like peptide 1 receptor-mediated cyclic AMP generation at Rab5 endosomal compartment. Mol Metab. 2017;6(10):1173-1185. doi:10.1016/j.molmet.2017.08.002.
- Müller TD, Finan B, Bloom SR, D'Alessio D, Drucker DJ, Flatt PR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2019;30:72-130. doi:10.1016/j.molmet.2019.09.010
- Maeng J, Lee K. Systemic and brain delivery of antidiabetic peptides through nasal administration using cell-penetrating peptides. Front Pharmacol. 2022;13:1068495. doi:10.3389/fphar.2022.1068495
- Shaji J, Patole V. Protein and peptide drug delivery: oral approaches. Indian J Pharm Sci. 2008;70(3):269-277. doi:10.4103/0250-474X.42967
- Zhou Y, Arribas GH, Turku A, et al. Rare genetic variability in human drug target genes modulates drug response and can guide precision medicine. Sci Adv. 2021;7(36):eabi6856. doi:10.1126/sciadv.abi6856